Breast Reconstruction
Information
What types of reconstruction can be performed after breast cancer?
Broadly there are two types of reconstruction, one is autologous meaning that your own tissues are used to reconstruct the breast and the other is implant based reconstruction where either a fixed volume implant or tissue expander is placed under your tissues.
Going ahead with implant based or Autologous based reconstruction is dependant on patient choice. It also depends on the patients body habitus; some patients will not have enough donor tissue to reconstruct the breast.
For the purposes of this leaflet we will discuss the use of the DIEP flap in breast reconstruction.
What is a DIEP flap?
DIEP stands for deep inferior epigastric artery perforator flap , and is tissue that is taken from the abdomen with its blood supply to reconstruct the breast. This is a long microsurgical procedure that can take up to 6 - 8 hours.
However its advantages include replacing like with like tissues that have same consistency and feel as the native breast. Furthermore the tissues will change as the patients body gains or loses weight. In contrast to a breast implant reconstruction that may eventually need replacing as it is a foreign body.
How is a DIEP flap procedure performed?
This is usually a two team approach with a breast surgeon performing the mastectomy and the plastic surgeon raising the flap from the abdomen.
Essentially the excess abdominal tissue is used to reconstruct the breast after mastectomy. It has to be carefully raised and the blood vessels that traverse across the rectus muscle are dissected free.
This technique is an evolution of the TRAM flap, which was a procedure where the entire muscle was taken with the abdominal fat. This is now rarely performed .
The flap is raised preserving the muscle and then transferred as as tissue to reconstruct the breast. One can also take the blood supply from both sides of the abdomen , a so called Bipedicled DIEP, this enables harvest of the entire abdomen to reconstruct the breast. But often just half or a portion of the abdomen in needed in most cases.
The abdomen is closed leaving a similar scar to a tummy tuck. If a DIEP flap is taken it is rarely necessary to place a mesh to support the abdominal wall.
How is the DIEP flap connected to the chest?
The blood vessels in the chest are prepared. These are the internal mammary vessels. Often a small portion of rib 2-3cm needs to be removed to access these vessels. If the patient has had radiotherapy these vessels can be friable and rarely additional vessels from the arm such as the cephalic need to be used.
The vessels from the DIEP flap are connected with small sutures under the microscope to the internal mammary vessels.
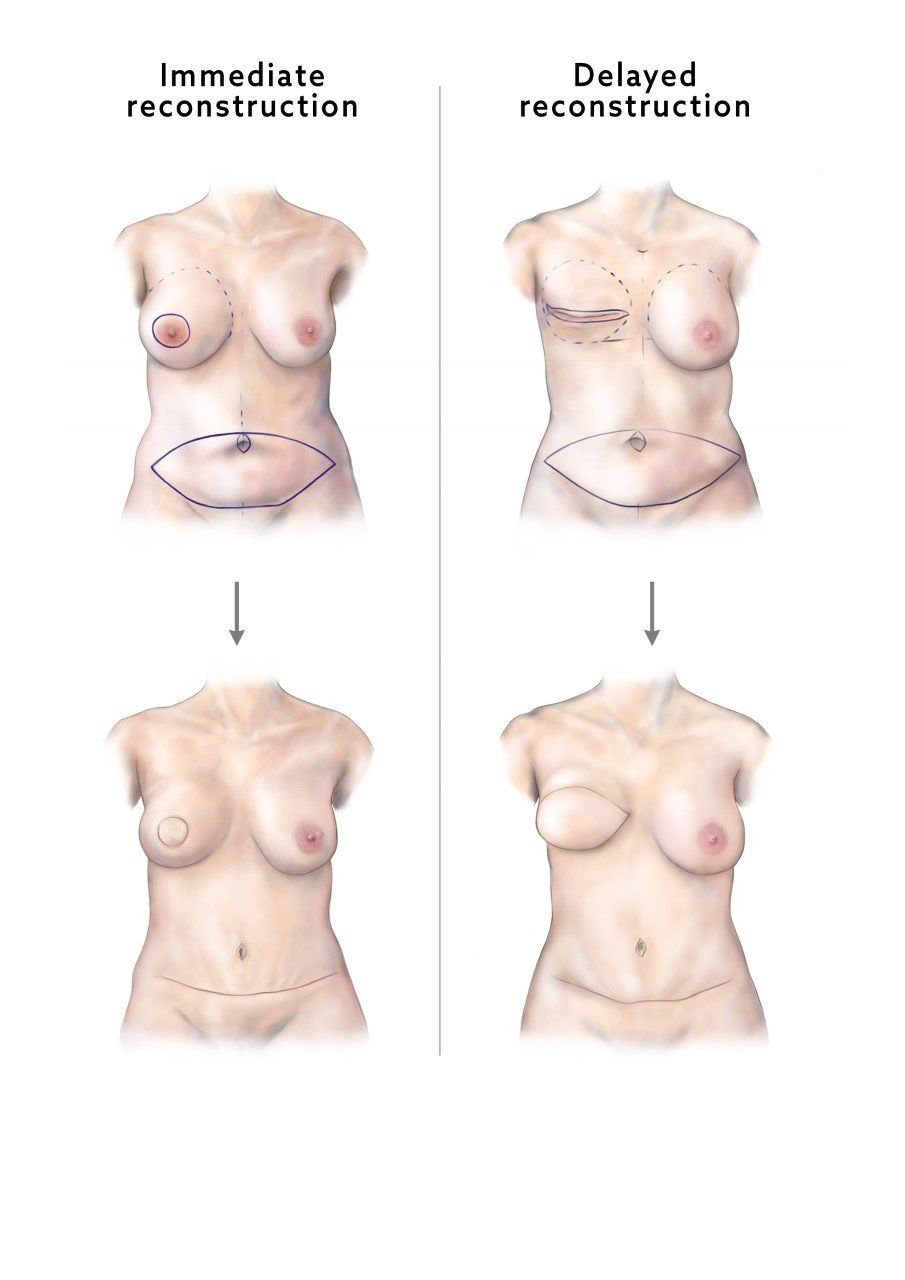
What is the difference between delayed and immediate reconstruction?
Some patients opt for delayed reconstruction and have a mastectomy first. In many cases however the reconstruction can be done immediately with the mastectomy. The DIEP skin paddle is larger in the delayed group as the mastectomy skin flaps are not preserved.
Who is ideal for a DIEP breast reconstruction?
Patients need a sufficient abdominal tissue. Previous C-sections do not contradict the use of a DIEP flap. If the patient has had previous open abdominal surgery a CT angiogram is performed to check if the blood vessels (perforators ) are present .
Studies have shown patient with a high BMI (above 30); there is higher risk of complications e.g wound break down and infection. In some cases we do perform immediate reconstructions in patients with a BMI of up to 35 but patients are told of the increased risk. Particularly in delayed reconstructions we advise patients to achieve a BMI less than 30.
What investigations do I need before a DIEP flap?
You will need some routine blood tests. And a CT scan of your abdomen to check whether you have adequate blood supply for the DIEP flap.
When can I have a DIEP reconstruction whilst on chemotherapy?
We usually wait 4-6 weeks after chemotherapy has finished before performing mastectomy and DIEP reconstruction.
When can I have delayed DIEP reconstruction after radiotherapy?
Most clinicians wait for around 12 months after radiotherapy as evidence points to lower complication and flap failure rates .
What is the inpatient stay like for a DIEP procedure?
It can be up to 5 days but due to our enhanced recovery protocol many ladies are going home earlier such as on day 3.
On the first postoperative night the flap is checked frequently and this is often the most sleepless and difficult night. After 48 hours flap observations are less frequent.
On day 2 most patients have their urinary catheters removed and are sitting up out of bed and able to walk on the ward. Pain catheters in the abdomen give good long lasting relief and are usually kept in for 48 hours.
What would you expect after DIEP reconstruction?
DIEP breast reconstruction is the biggest operation in the journey to rebuild the breast after cancer. Depending on what the patient wants in terms of size, we often try to match the contralateral breast. This sometimes is not possible and smaller secondary procedures are needed. Patients will often need a secondary operation on the contralateral side to reduce and lift the breast (breast reduction or mastopexy).
If there are any contour irregularities in the reconstructed breast these can also be addressed in smaller operations.
What are the complications after DIEP reconstruction?
There is a 1-4% risk of total failure. This risk is increased in patient with high BMI. There are risks of infection, wound breakdown at the breast and abdomen, poor scarring. Patients sometimes will need to go back to theatre in the acute period for any of these risks and also if there is compromise to the blood supply of the DIEP flap.
In rare cases you may get an abdominal bulge called a hernia, this can be due to a weakness in the abdominal wall. If troublesome it may require secondary surgery.
Can I get my nipple reconstructed?
Nipple reconstruction can be performed as the final stage of the breast reconstruction journey. A new nipple can be made from local tissues under local anaesthesia. Once the new nipple has healed the areola can be Tattoo’d to match the contralateral breast. If the colour fades this procedure can be repeated.
What should I wear post operatively?
A well fitted supportive sports bra is recommended to support the reconstructed breast. We also recommend well fitted pants to support the abdomen which will be bruised and somewhat tender in the first couple of weeks after surgery.
Acknowledgements : Miss Julia Ruston for the clinical images she has drawn.
Acknowledgements : Miss Julia Ruston for the clinical images she has drawn.